
The 2x Referral Bonus Event Is Now On! More Info ➡️
SAVE 10% OFF First Order With Coupon Code: WELCOME10
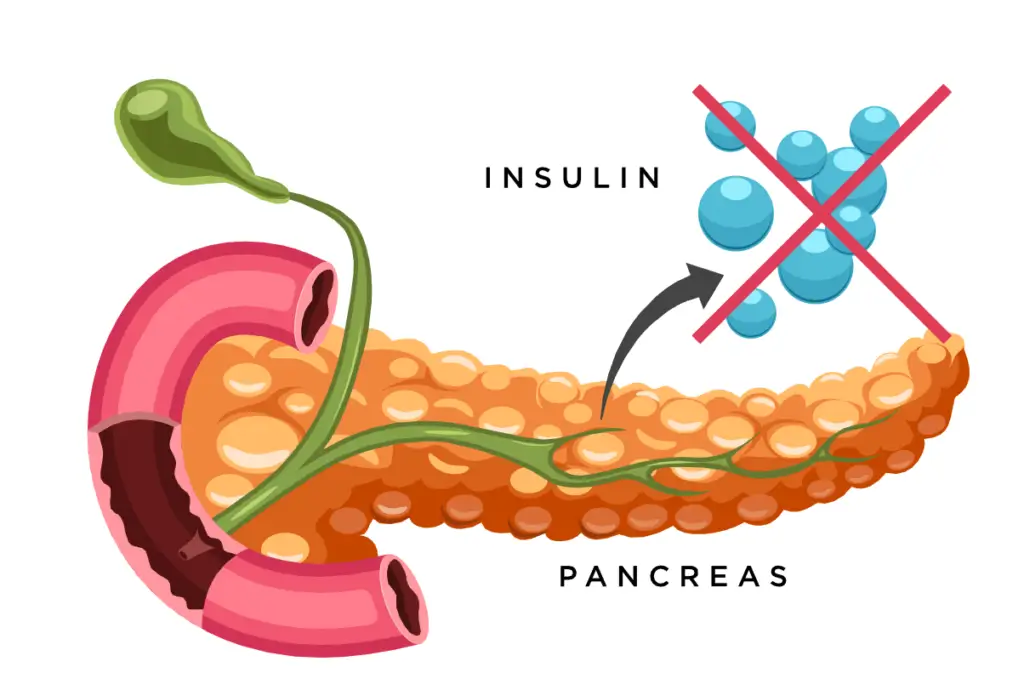
Diabetes is a metabolic disorder characterized by high blood sugar levels that result from a problem with insulin function. Either your body does not produce insulin, which is called Type 1 diabetes, or your body does not properly use the insulin that it does produce, which is called Type 2 diabetes. Type 1 diabetes is also sometimes referred to as insulin-dependent diabetes.
Insulin is an important hormone produced in your pancreas that regulates your metabolism by helping your body use the sugar from your food as energy for your body. It is involved in the breakdown of sugars, fats, and proteins as well as the control of your blood sugar levels. Insulin balances your blood sugar levels, decreasing them if they become too high. It absorbs sugar from your bloodstream, processes it, and allocates it to your fat, liver and skeletal muscle cells. It also helps to block the production of sugar in your liver and the release of sugar from your liver into your blood. Insulin also signals your body to store the extra sugar when there is an excess of it in your blood. The stored sugar is released again only when your blood sugar levels drop, such as between meals or when you engage in physical activity.
Insulin was first discovered by Frederick Banting and John Macleod at the University of Toronto in 1923. The Nobel Prize was awarded to Banting and Macleod for their discovery of insulin.
The pancreas is an organ that is important in digestion and blood sugar control. It produces and releases a variety of digestive hormones into the bloodstream and digestive system. It is a large, flat organ, about 6 inches in length, and is found in the upper left part of your abdomen behind your stomach. There are about three million cell clusters in your pancreas called pancreatic islets (or islets of Langerhans), which consist of four types of cells. Each type of cell releases one of four different hormones involved in the regulation of blood sugar levels:
When your blood sugar levels get too high, the pancreas secretes insulin. When your blood sugar levels get too low, the pancreas secretes glucagon.
Beta cells are the most essential cells in your body for the proper regulation of blood sugar. Their primary function is to store and release insulin. When your blood sugar levels are high, your beta cells secrete insulin into the blood. When your blood sugar levels are low, the release of insulin is stopped. Beta cells can respond rapidly to spikes in blood sugar levels by releasing their stored insulin into the blood, and at the same time produce more insulin.
Beta cells also play a crucial role in the development of diabetes. In those who have diabetes, it is thought that either their beta cells have been destroyed, or they have become non-functional because of an auto-immune attack.
Insulin dysfunction is the hallmark of diabetes, as it leads to abnormally high blood sugar levels that have profound effects on your quality of life. It is a chronic and often debilitating disease that can be fatal. As of 2016, 422 million people worldwide have diabetes, with type 2 diabetes making up about 90% of the cases. The World Health Organization predicts that by 2030 the number of people with diabetes will be more than double that number.

These symptoms may develop quickly over a few weeks or months for those with type 1 diabetes. Symptoms may come on more gradually and be more subtle, or even absent, in those with type 2 diabetes. If your diabetes is left untreated, more serious complications can occur, including diabetic ketoacidosis (DKA), hyperosmolar hyperglycemic state, blindness, amputation or even death. Other long-term complications may be cardiovascular disease, kidney disease, stroke, foot ulcers, and eye damage.
Diabetes is characterized by high blood sugar, which can be diagnosed by any one of the following:
Currently, there is no known cure or preventive measure for Type 1 diabetes. Type 2 diabetes can be prevented to some degree by maintaining healthy body weight, getting regular physical activity, and consuming a balanced diet.
Type 1 diabetes, sometimes called insulin-dependent diabetes or juvenile diabetes, results from your pancreas’ inability to produce the required insulin for your body because of the loss or dysfunction of beta cells in your pancreas.
The exact cause of type 1 diabetes remains unknown, although it is believed to involve a combination of environmental and genetic factors. The underlying mechanism of beta cell problems appears to involve an auto-immune attack. Auto-immune reactions occur when your body’s own defense system mistakenly targets its own cells and destroys them. In the case of diabetes, the immune system may target and destroy the beta cells in the pancreas.
Type 1 diabetes must be managed with daily insulin injections and meal planning to lower and control blood sugar levels.
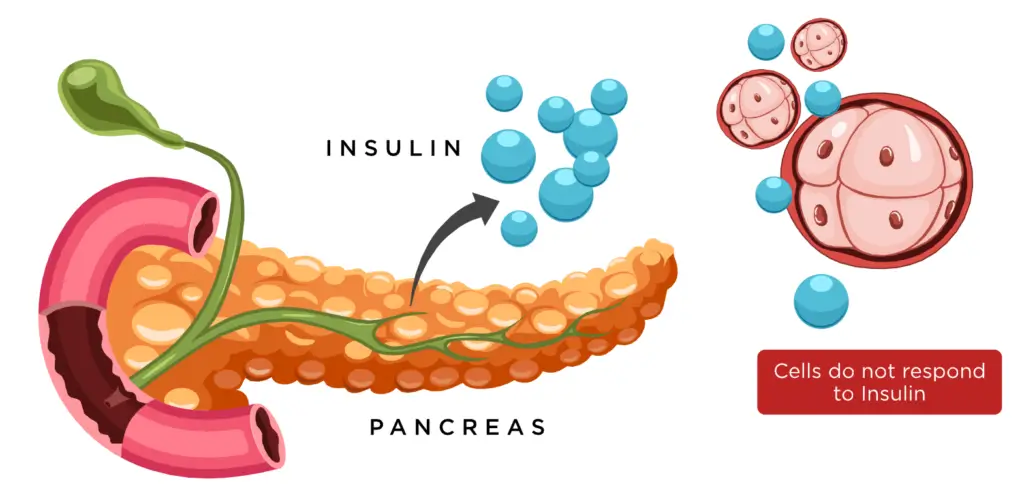
Type 2 diabetes, which accounts for nearly 90% of all diabetes cases, is sometimes referred to as adult-onset diabetes. It occurs when your body cannot properly use the insulin that is being produced. Type 2 diabetes is also called insulin resistance. As the disease progresses, insulin production may stop completely.
Typically, it develops after age 35, which is why some refer to it as adult-onset diabetes, but recently there has been a growing number of young people developing type 2 diabetes. Some people are more at risk of developing type 2 diabetes than others, due to their genetics, but it primarily develops as a result of lifestyle factors, such as overeating, having excessive body weight (obesity) and not getting enough exercise.
Depending on the severity of type 2 diabetes, it may be managed through a healthy diet and regular exercise, or it may also require antidiabetic medications or insulin to help regulate high blood sugar levels.
Gestational diabetes is a third type of diabetes. It is a temporary diabetic condition that occurs when pregnant women, who did not previously have a history of diabetes, suddenly develop high blood sugar levels during pregnancy. It affects between two to four percent of all pregnancies. It is caused by not having enough insulin, which can lead to insulin resistance. Some risk factors for gestational diabetes include being overweight, having gestational diabetes in previous pregnancies, having polycystic ovarian syndrome, and a family history of type 2 diabetes.
Gestational diabetes increases the risk of depression, pre-eclampsia, and Caesarean section. Babies that are born to mothers who have inadequately treated their gestational diabetes are at an increased risk of having low blood sugar.
This is due to the mother’s high blood sugar crossing into the baby’s bloodstream and prompting the baby’s pancreas to start producing insulin. Babies born to mothers with gestational diabetes may also become too large, and have an increased risk of jaundice. In the long-term, these children are also at a higher risk of becoming overweight and developing type 2 diabetes later in life.

An insulin analog is man-made insulin produced using recombinant DNA technology. The human insulin gene is inserted into E. coli bacteria, or into yeast, which then produces insulin for human use. This synthesized insulin is sometimes given minor structural changes to give it specific characteristics. This is how different insulin, such as NPH insulin, is made. However, once the insulin is absorbed by the body, it acts just like naturally occurring, human insulin.
This technology has been used to produce two main types of insulin analogs: those that are more rapidly absorbed and act faster, and those that are released slowly and work over the course of the day. The faster-acting insulin analogs are designed to protect you against mealtime spikes and fluctuations in blood sugar levels. These are called mealtime, or bolus insulins. Insulins that have an extended duration of action are used for maintaining blood sugar levels throughout the day and night. These are called basal, or background insulins.
Recombinant technology has almost completely replaced insulin produced from animals, such as pigs and cows. Before synthesized insulin, pig pancreases were used to produce usable insulin. It took two tons of pig pancreas to produce only eight ounces of purified insulin.
Basal-Bolus therapy involves combining a longer-acting, or basal insulin analog, together with separate injections of a shorter-acting, or bolus insulin analog.
The role of basal insulin, also known as background insulin, is to keep blood sugar levels stable throughout the day and allow your body to take in sugar used for energy for all of the functions needed to support daily life. It acts over a relatively long period of time and is usually taken once or twice a day. Either long-acting or intermediate-acting insulin analog is used as part of basal-bolus insulin therapy.
The other part of basal-bolus insulin therapy includes bolus insulin, which is specifically taken at mealtimes to prevent the blood sugar spikes your body experiences after meals. It needs to act quickly, therefore short-acting and rapid-acting insulin analogs are used in basal-bolus insulin therapy.
For basal-bolus therapy, you generally take multiple daily subcutaneous injections, which better replicates the way naturally occurring human insulin works in your body. A healthy pancreas naturally releases more insulin during meals, to combat the blood sugar level spikes that occur during and after mealtime. A basal-bolus regimen allows you to closely match how a non-diabetic body would release insulin. It also allows for flexibility, for when you would like to take your meals. Basal-bolus therapy can prevent blood sugar highs and lows, which allows you to feel better throughout the entire day.

There are four major types of human insulin analogs that are available, which are categorized based on how fast they begin working:
There is a fifth type of insulin analog, which is a combination of shorter acting insulin and longer-acting insulin. This type of insulin is called Pre-Mixed insulin, but many refer to it as simply an “insulin mix.” All of these analogs are closely related to naturally occurring insulin in structure and in the ability to control blood sugar levels. Insulin analogs differ from naturally occurring human insulin in their onset of action and in their duration of action.

Rapid-acting insulin analogs are taken as a bolus or mealtime insulin, right before meals, to cover the blood sugar elevation that results from eating. They typically begin to work in about 10 to 30 minutes, with a peak action around 30 minutes after being taken. Their duration of action lasts approximately 3 to 5 hours.
The first insulin analog that was developed was rapid-acting Humalog (insulin lispro). Rapid-acting insulins are all rapidly absorbed due to their small structural units that do not combine into larger more complex molecules, as naturally occurring human insulin can. Some examples of rapid-acting insulin analogs are:
Intermediate-acting insulin analogs can be used as a basal or background insulin, which is used for day and nighttime protection against blood sugar elevations. When using a basal-bolus regimen, they protect you from blood sugar elevations that occur when rapid or short-acting insulin analogs finish working. They are usually taken twice a day and are often combined with a shorter acting insulin. They have a typical onset of action around 1.5 to 4 hours, a peak action that occurs around 4 to 12 hours after injection, and they last about 24 hours. NPH insulin, also called as isophane insulin, is an example of a commonly used intermediate-acting insulin analog. It has small proteins called protamines added to it to slow down its onset and extend its duration of action. Some brand names of NPH insulin are:
Short-acting insulin analogs are also called bolus insulin analogs, which are used to cover your mealtime insulin needs, although they work slightly slower than rapid-acting insulins. They are used for meals eaten within 30 to 60 minutes after being injected. They usually start to work about 30 minutes after subcutaneous injection, with a peak action that occurs in about an hour, and a duration that lasts about 12 hours. Regular insulin also called neutral or soluble insulin is an example of a short-acting insulin analog. An example of a short-acting, brand name insulin is Humulin R.
Long-acting insulin analogs are also used as basal or background insulin, which covers insulin needs for the entire day, as well as overnight. They begin to work in about 1 to 4 hours, with a relatively minimal peak of action. They tend to last about 24 hours or more. Examples of long-acting insulin analogs are:
Premixed insulin combines two types of insulin analogs together: basal insulin that helps you control your blood sugar all through the day, and bolus insulin for the control of blood sugar levels at meal times. Pre-mixed insulin is often referred to as simply a “Mix” insulin.
Premixed insulins were initially developed to simplify your diabetes management and insulin dosing. Premixed insulin combines shorter and longer-acting insulins in one cartridge, pen or vial. With the proper ratio, it gives you quick coverage for a meal plus longer coverage for other times of the day. They are typically injected two or three times a day, before mealtime. While there is a variety of ratios of premixed insulin available, the ratios are not individually customized.
The pre-mixed solutions come in ratios of 25/75, 30/70, 40/60 and 50/50, with the faster-acting insulin generally in lower relative amounts than the longer acting insulin analog.
Unlike much oral antidiabetic medications, insulin currently cannot be taken orally and needs to be taken as a subcutaneous (under the skin) injection. Like most proteins you eat, insulin gets reduced into tiny fragments once it reaches your stomach and intestines. When this happens, insulin’s therapeutic activity is lost. Currently, there are two main ways to administer your insulin analogs, either with an insulin pen or with a syringe.

If your child or teen has been diagnosed with diabetes, the next step is to create a diabetes management plan to help manage your child’s condition in order to keep them healthy and active. To help minimize the symptoms of high blood sugar levels, insulin treatment is usually started as soon as possible after diagnosis. Whatever the age of your child, the aim is usually to find an insulin replacement that can help control your child’s blood sugar levels. Children with diabetes (especially type 1) are dependent on insulin for survival and should have access to adequate amounts of at least Regular and NPH insulin. Most insulin therapies can be used for children over the age of 4. Talk with your doctor about the specific types of insulin that best suit your child’s specific insulin needs.
Household pets, like cats and dogs, can also develop diabetes just like people do. Other animals like pigs, horses, and apes are also susceptible to developing diabetes. Just like with people, cats and dogs can be treated with insulin therapy. The most common form of diabetes in dogs is Type 1 diabetes, in which they would require daily insulin injections. Type 2 diabetes, on the other hand, is the most common form of diabetes found in cats.


It is a good idea to practice loading your syringe and using an apple or orange to practice giving injections until you feel you are ready to give your cat or dog an insulin injection. There are many different kinds of syringes, needles, and types of insulin, so make sure you get the right size and type as recommended by your veterinarian.
The starting dosage of insulin is typically around 0.25 units per pound, and they are usually given twice a day, with larger dogs needing closer to 0.5 units per pound. The general idea is to start with a low amount of insulin, and then gradually give more if your pet needs it. Injections are usually made near the middle of the back (spine), either behind the shoulders or in front of the pelvis, alternating sides between injections.
Using your free hand, pinch a fold of skin and gently insert the needle into the center of the fold. Once the needle is in the skin, gently push the plunger in. Make sure to speak with your vet beforehand about proper injection techniques, and always follow their directions carefully.
Insulin Outlet
My Account
Customer Service
Email: info@insulinoutlet.com
Fax: 1-888-804-1287
Hours Of Operations
Mon-Fri: 9AM – 11PM
Sat: 10AM – 4PM
Sun: 9AM – 3PM
Intellectual Property Rights: All logos, trademarks, and brand names displayed on insulinoutlet.com are the property of their respective owners. Insulinoutlet.com uses these logos and trademarks solely to identify the products we carry and to provide accurate information to our customers. The use of these logos does not imply endorsement or sponsorship by the respective owners. If you believe that any material on our site infringes your intellectual property rights, please contact us immediately at help@insulinoutlet.com so that we can address your concerns promptly.
Copyright © 2025 Insulin Outlet – All Rights Reserved



You can see how this popup was set up in our step-by-step guide: https://wppopupmaker.com/guides/auto-opening-announcement-popups/
We are experiencing a shortage of Ozempic pens. To be able to serve all our customers and to make sure all our customers do not miss their dose we are limiting purchases to 1 pen per order for 4mg pens.
This medication requires to be shipped cold. The cold shipments are closed for the holidays between December 19th, 2022 and January 3rd, 2023. You can place the order however your card will not be charged until the item is ready to be shipped.
Unfortunately, our supply has slowed down with the Ozempic 2mg/1.5ml pen (weekly doses of .25mg and/or .50mg). While we are still receiving shipments of these Ozempic pens, they are not at the same supply levels as before. There will be a slight delay in shipments as it could take up to 2 weeks for the orders to be shipped. We apologize for any inconvenience.
Due to potential shortages of Ozempic in Canada, we are following the recommendations from the Canadian Ministry of Health, and will not be able to take any new customers for the time being. We apologize for the inconvenience.
We can still process refills for existing customers.
Our team is working around the clock to find a solution to this current situation.
If you do have any questions or concerns, please do not hesitate to reach out to us.
We are experiencing a shortage of Ozempic pens. To be able to serve all our customers and to make sure all our customers do not miss their dose we are limiting purchases to 2 pens per order for Ozempic 2mg pens.
By checking this box, you are opting in to receive SMS (text) messages from us. We will send you text notifications, updates, and may engage in SMS conversations to provide support or gather necessary information for your account. Your mobile number will not be shared with third parties and will be used in accordance with our privacy policy. Message and data rates may apply. You can reply STOP anytime to opt-out of SMS communications at anytime.
[Pharmacy_login]
Cold Medication Shipments
Please be aware that cold-chain shipments, including products like Ozempic, Mounjaro, and Insulin, will not be available for delivery from December 20th through January 1st.
Dry Medication Shipments
For dry medication shipments, including pills and tablets, there will be a brief interruption in service from December 23rd through December 28th. During this period, we will not be able to process or ship these items.
We kindly request that you plan your medication needs accordingly to ensure you have an adequate supply during this short shipping pause.